



PLANNING TEAM:
The course was planned in the UK by Dr Ruth Spencer (anaesthetics) and Mr James Berwin (orthopaedics)
At each stage it was discussed and approved by the Ethiopian steering team, principally Mr Bekalu Wubshet (orthopaedic attending) but also Mr Biniyam Biresaw (orthopaedic attending) and Mr Bini Teshom (Head of Orthopaedics)
In addition to the planning team, the following people formed the course faculty and undertook all the teaching of the first course and subsequent training the trainers.
Mr David Woods (Orthopaedic Consultant Swindon)
Mr Gwithyen Silk (Orthopaedic Registrar Severn Deanery)
Mr Aveek Mitra (Orthopaedic Registrar Severn Deanery)
Mr Dan Yeomans (Orthopaedic CT2 Severn Deanery)
Dr Lyndsey Hewiston (Cardiology Registrar Severn Deanery)
Dr Yiannis Vyrides (F2 doctor in Swindon)
Background;
This PTC course came about following a request from the senior surgeons at the newly built University hospital in Bahir Dar.
A project with World Orthopaedic Concern was already in progress and working towards establishing an on-going link with the Severn Deanery orthopaedic surgeons. Visits had already been made by Mr David Woods in January 2019 and by a team of orthopaedic surgeons later in February. As part of the third visit, a formal PTC course was requested.
Bahir Dar is a town approximately 580km north of Addis Ababa, in the Amhara region, near Lake Tana and the Blue Nile river. There are two hospitals; Felege Hiwot, the Government Hospital and now Tibebe, the newly built University Hospital. These two centres serve an estimated population of 17 million from the entire Amhara region, not just the immediate town population of 650,000 .
At the last visit, Tibebe Hospital was still under construction. Since then, they have fully opened, including an impressive new Emergency Department. A separate educational facility has been built to include a nursing school as well as medical student and doctor training. A library and new research facility are also under construction.
The majority of the resident and attending orthopaedic surgeons have transferred to the new hospital. As such, this was the perfect time teach and embed good resuscitation training.
Practicalities:
The teaching facilities provided were extremely good with reliable laptop projection, a good room for lectures and plenty of space in additional rooms for skills stations, including a simulation model.
Refreshments and lunch were also reliably provided.
Transport for the faculty from the hotel was unfailingly punctual and well driven in a vehicle with seat belts.
The hotel was comfortable with good food and constant hot water.
These aspects were run like clockwork and all organised by the Ethiopian team.
Teaching:
We taught 21 people on the first course, selected 6 instructors and then taught another 26 on the second course. The pre-course MCQs showed a high educational level, but a lower level of confidence. Both post course MCQs showed that all candidates had been brought up to the same very high standard and that confidence had dramatically improved.
The standard was such that leadership during trauma calls was a concern for them. The most appreciated part of the course was therefore the scenarios as that allowed them to bring together all that they had learned to put into practice. The improvement in the ability to organise their approach was incredible.
We were also stunned by just how well the new instructors ran the second course. They had thoroughly grasped all the principles and were absolutely brilliant in teaching the information. They also organised themselves really well and kept to time. It was an overwhelming pleasure to see how fantastically they had on taken all the new information.
The local organising group of three doctors in Ethiopia were fundamental to running this course successfully. They were clear about what they wanted and after understanding the pattern of the 2:1:2 course went on to recruit doctors and nurses for both courses.
They were also clear that both days needed to be attended for certification and that anyone selected to do the “training the trainers” day would need to be available for all 5 days. They were incredibly organised and delivered 21 participants on the first course and 26 on the second.
They sent photos of the training facilities which were perfect for the teaching, were accurate and available to us exclusively and on time.
They were quick to communicate about facilities available and to let us know what equipment they had /lacked.
It is absolutely the most organised and efficient local group I have had the pleasure of working with.
In the meantime, James Berwin and Ruth Spencer prepared the course to match the requirements of Bahir Dar. Some copies of the manual were printed in the UK as were all the MCQ / answer sheets and registration forms. We were correctly assured that all candidates had laptops and access to the online manual and slides.
The first two days of the course ran along the lines of an expected PTC course, with a the following important exceptions.
1. We were specifically asked to teach a session on CPR. We included paediatric CPR and combined it in two parallel and very practical sessions with “helping the choking child.” Playing the tune “Staying Alive” to teach the correct rate for chest compressions was very popular
2. As the hospital does not have interosseus needles, we chose to teach difficult venous access by using a cut down. We showed a very clear video and then used one of us as a model to demonstrate landmarks. This is the method they resort to when unable to find a vein, so we felt it right to teach.
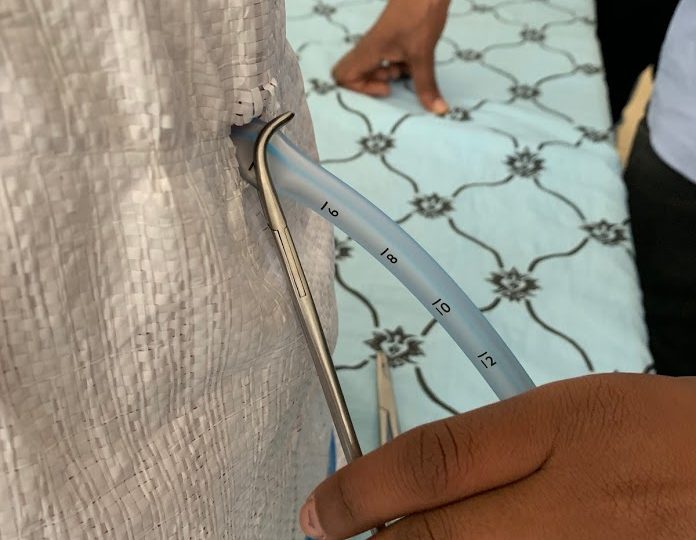
3. They were keen to practice chest drain techniques but not to obtain and kill a goat. As such, we set about improvising a model that could be used to teach and came up with the idea of a bin with palpable slats, covered with plastic sacking and lined with foam to simulate the correct depth. All these items were bought in the local market and then built into two models by Yiannis. They worked perfectly, cost next to nothing and can be reproduced for further teaching later. A session on identifying the safe zone landmarks was also held using one of us as a model.
4. On the first course, we had many of the senior doctors in the hospital attending. They had already demonstrated great knowledge, so we took the risk of holding small discussion groups on day 2. We approached it with some trepidation, but it was truly informative and will we hope lead to great progress.
In groups of five, each containing surgeons, anaesthetists, nurses and a senior member of both the UK team and the Ethiopian team, we invited them to discuss the practical issues that prevent successful trauma management at their hospital.
With little input from the UK team, they were able to identify many issues. These included:-
No warning that an ambulance was about to arrive
No trauma call and insufficient help in ED
Inability to intubate a patient in ED who would need to be transferred to theatre for an anaesthetist to do it there.
Overwhelming paperwork leading to very poor review of ED patients after initial assessment.
Poor handovers at shift change times and poor collaboration between specialties.
Difficulties in obtaining blood, especially in the summer, as almost all donations come from university students.
Poor drug prescribing, illegibility and duplication of paperwork. Multiple drug errors.
A list of practical issues was made and submitted to Mr Bini Teshom. With great humility, he accepted every criticism and at the end of the course made an inspirational speech about how they would tackle these problems and resolve the issues that he described as “being in their own hands”
Whilst an unusual step to have taken, their approach was so open and honest that they have an impressive will to acknowledge problems and a real appetite to change for the better. It is likely that this group discussion will ultimately lead to extremely positive advances in trauma care.
Programme:
Course 1: Trained 21 people
These were extremely knowledgeable people whose initial MCQ scores ranged from 11-19.
Post course, the scores ranged from 18-20 with 8 people scoring the full marks.
Graph of MCQ scores: Users/ruthspencer/Desktop/Day 1:2..jpg
Course 2 Trained 26 people
Pre course MCQ was more spread out ranging from 7-19
Post course scores were 13-20 with 12 people scoring the maximum.
Graph of MCQ scores /Users/ruthspencer/Desktop/Day 4&5.jpg
Confidence scores all increased. The full data on each individual confidence score for the scenarios quoted is attached in the spreadsheet in both Numbers and Excel format. It is appended separately. Below are some pdfs.
/Users/ruthspencer/Desktop/PTC Bahir Dar All data.pdf
/Users/ruthspencer/Desktop/PTC Bahir Dar MCQ Marks, confidence matrix and feedback Day 1:2.pdf
/Users/ruthspencer/Desktop/PTC Bahir Dar MCQ Marks, Confidence matrix and feedback Days 4:5.pdf
The appended spreadsheet includes all the comments on most useful things learned and changes made.
The over riding theme was of organisational improvement, the establishment of trauma teams and the understanding of the ABC principle
This was a highly successful course and has come at the perfect time for this hospital. After teaching on days 4/5 the new trainers had already selected the next 6 people to do the instructors course and had set a date the following week to teach them.
I am confident that they are able to keep the ball rolling. There is also a real will to improve, backed up at the highest level.
In the future, there will be further visits from the new Severn Deanery orthopaedic link which will be an on-going project.
Two of the Ethiopian team leads will be coming to the UK for orthopaedic training, a Bristol visit and to attend a national conference in Edinburgh.
The course could have been more effective if there had been more nurses and anaesthetists. It was slanted heavily towards surgery, orthopaedics in particular. However, they have now recognised the value of inter disciplinary working and it was noted that their selection of the next instructors included representatives from both those specialties and also a general surgeon. They had already recognised the problem!
Another difficulty is that only one person was able to attend from the Government hospital Felege Hiwot. The distribution of work in this area now that there is a newly built hospital will be an issue and a difficult political problem. It would be preferable that the old Government hospital doctors / nurses should also be trained in PTC.
As is often the case, the anaesthetists are clinical practitioners and not doctors. The only doctor anaesthetist in the entire area (one of 45 in the country) attended on one day. He is hoping to gain a residency programme in the area soon, but he is fighting a somewhat lone battle for this.
All post course evaluation comments are on the spreadsheet. Most appreciated were the scenarios and the skills stations.
James Berwin and David Woods for introducing the possibility of PTC to an on-going orthopaedic project and for their tireless work in driving this endeavour forward.
It is very satisfactory that repeat visits will occur and that such a friendly and productive link has been made.
Involve more nurses and anaesthetists in addition to surgeons
Ensure training occurs at the Government hospital as well as the University one.
Support the formation of multi disciplinary trauma teams
Teach effective trauma leadership.
Support the residency programme request for anaesthetic doctor training.
This was a well-organised course, with detailed planning, experienced instructors and a thorough assessment. It could be duplicated elsewhere.
One of best training i had been involved so far. I acquired new basic lifesaving skill and elaborated what in have before! Great thanks to PTC team!